First came the headaches, a feeling of pressure in the head. Then, Shane Christie started experiencing macabre hallucinations of his own death. Later, the once sociable New Zealand rugby player started getting into arguments with loved ones and towards the end paranoia consumed his trust, making him fearful and depressed.
By the time Christie took his own life aged 39 in August – some 10 years after he first started experiencing the headaches – he was almost unrecognisable to those closest to him.
Holly Parkes, Christie’s former partner, looked after him in the last year of his life. Parkes says she felt desperate and alone watching Christie disappear further into the illness he believed was caused by multiple head injuries.
“I would get in the car, and I would cry, and I would call people… I would speak to every friend that I had … I called the brain injury trust…I was trying to speak to people in the [US], like, what do we do? How can I help him?”
Christie suspected he suffered from chronic traumatic encephalopathy (CTE) – a progressive brain disease associated with head impact, which can be diagnosed only posthumously. His symptoms were consistent – fatigue, mood and personality changes, confusion, paranoia, anxiety, headaches and suicide. His case has been referred to the coroner.
Christie has donated his brain to New Zealand’s human brain bank, which is studying athletes’ brains for signs of CTE. If diagnosed, he could become the second New Zealand rugby player after Billy Guyton confirmed to have the disease, and with it, Christie’s desire to raise awareness about CTE and force changes in New Zealand’s rugby industry, could take on new life after his death.
From the stadium to the shadows
Before his symptoms took hold, Christie had been a passionate rugby player – playing domestic competitions and Super Rugby, and representing New Zealand in the Māori All Blacks and All Blacks Sevens.
To those closest to him, he was a lively, honest and forgiving man.
“He loved his friends, loved his family … was very trusting of people,” Parkes says. “He didn’t make his life more complicated than it needed to be. He just focused on big things.”
But life did become complicated for Christie. During his career, he experienced multiple impacts to his head, the accumulated effects of which took their toll.
In 2016, during his stint as co-captain of the Highlanders he took a significant blow during a game against the Kings in South Africa. Christie was flown home and was “alone in the dark for two weeks”, Parkes said. “He cannot even look at the window … because the light is so bad.
“He notices big changes in himself and is already asking for help but he’s being offered nothing, from anyone.”
Craig Morice, a Nelson-based lawyer who became friends with Christie, first got to know him in 2017, when he was brought on pro-bono to help with Christie’s retirement negotiations with New Zealand Rugby (NZR) and the New Zealand Rugby Players Association.
The two groups were “taking their time to assist him adequately, both in respect of specialist medical care and working out what his future options were” Morice tells the Guardian.
It took months of pushing NZR to secure Christie a specialist neurologist appointment, Morice said, which concluded that, due to the level and number of concussions he had sustained, Christie should retire from rugby immediately.
In 2018, Christie retired, citing ongoing effects of his head injuries but he expressed serious concerns about the handling of his case and the governing body’s processes for dealing with players experiencing concussion.
NZR agreed to carry out an independent review of Christie’s medical care and to include a set of recommendations in respect to dealing with players with concussion and rugby. The report was completed in 2019 but NZR did not make it public, saying it risked identifying players or medical professionals.
“Shane was distraught because these recommendations can only make their game safer,” Morice said. “If you can’t release recommendations, how on earth does the public know what they are? How do you see whether a body is implementing them?”
When Billy Guyton, a rugby player and friend of Christie’s took his own life after battling CTE in 2023, Christie’s resolve to see change happen deepened. He started the Billy Guyton Foundation to highlight the risks of repeated head impacts.
Christie saw himself in Guyton, and became convinced he too was suffering from CTE, Morice says. But his friend’s death also accelerated his own decline – Christie became more erratic, more hardened in some of his paranoid and conspiratorial beliefs and eventually, suicidal.
The fun-loving friend with whom Morice used to share a meal every week “was not the same person” by 2025, Morice says.
Despite his decline, Christie’s messages remained – to see better support for players and retirees and, in particular, a desire to see NZR and the players association formally acknowledge a link between degenerative brain diseases like CTE and the game of rugby, just as NFL representatives in the US had done in 2016, Morice said.
In 2023, the NRL and Football Australia also acknowledged the links.
“But New Zealand Rugby and the players association – they won’t acknowledge anything,” Morice said. “They will be on the wrong side of history on this issue, and the point is, we should be doing more for these people now.”
The players association was not available for comment.
In a statement, NZR said player welfare was “at the heart” of everything it does. It said it has been “at the forefront of concussion initiatives globally”, including education programmes, research into the long-term effects of head injury and establishing a prevention and management plan for concussion.
“We have publicly acknowledged that there is an association between repeated head impacts and CTE,” it said, adding its focus has been on reducing the risk of head injury.
“However, this is a complex issue and the science is evolving. NZR does not believe that enough research using study designs that would support causal statements has been done yet to confirm a causal link between head injuries and CTE.”
NZR said the report into Christie’s care did not find fault but NZR was making progress towards a series of its recommendations, including around support for former players, medical care and communication.
NZR would not discuss Christie’s case, but said “our rugby community remained committed to providing him with ongoing support”.
Those words anger Parkes, who says she watched Christie and Guyton “be cast aside” from the sport they loved, with no information or ongoing support and treatment.
Rugby is a beautiful sport, Parkes says, one that can offer social mobility in New Zealand, make players money and turn them into national heroes.
“But when you’re not in the stadium as a gladiator … if you’re not the strong, powerful person that they pay you to be … you’re left in the dark, alone,” she says.
Brain research could keep legacy alive
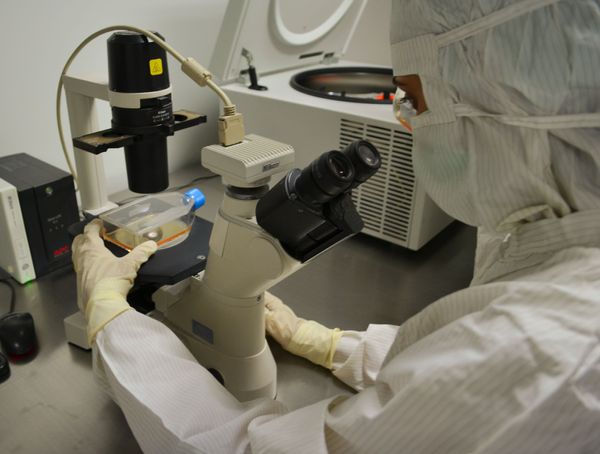
At the University of Auckland’s centre for brain research is a large laboratory, where researchers examine the donated brains of more than 1,000 people.
In one aisle, a pair of researchers dab at thin glass sections containing cerebellum, which spreads out like intricate botanical ink drawings. In other areas, scientists are reprogramming cells into neurons, to watch how they may react to injury.
It is here Guyton’s CTE was discovered, and where Christie’s brain will be investigated.
Dr Helen Murray, a senior research fellow at the centre and former national ice hockey player, says CTE is complex and there is no way to tell how prevalent it is among athletes or the wider public. It is also extremely challenging to diagnose CTE during life, because the symptoms overlap with other diseases.
While not every contact sport player will develop a brain condition, the risk is higher for those groups, Murray says.
Researchers are only just starting to understand CTE, she says, but what they do know is a protein called tau overdevelops in the brain in areas where there have been impacts. It clumps up and chokes off blood vessels and the neural pathways.
“It looks like these big flame-shaped fibres that’s all over the cells,” Murray says. “Once it’s formed, its really hard to get rid of.”
Murray hopes her research will in time inform ways to minimise the risks of developing CTE – whether that means through shorter sport seasons, better aftercare or delaying contact sports for children.
Christie’s loved ones hope his final big play – donating his brain to research – will push his desire for CTE awareness to the fore.
“I think people weren’t actually listening when he was trying to explain things before,” Parkes says. “But as the years go on, the things that he said in the final years of his life may become even more poignant and even more profound.”
In New Zealand, Lifeline: 0800 543 354. Suicide Crisis Helpline: 0508 828 865 / 0508 TAUTOKO (24/7). This is a service for people who may be thinking about suicide, or those who are concerned about family or friends. Depression Helpline: 0800 111 757 (24/7). In Australia, the crisis support service Lifeline is 13 11 14. In the UK and Ireland, Samaritans can be contacted on freephone 116 123, or email jo@samaritans.org or jo@samaritans.ie. In the US, you can call or text the 988 Suicide & Crisis Lifeline at 988 or chat at 988lifeline.org. Other international helplines can be found at befrienders.org