
Anthony Albanese and state premiers will negotiate a plan to radically overhaul Medicare on Friday as new figures show Australians’ waiting times for health care have blown out since the pandemic hit.
Significant delays are emerging across all three parts of the health system funded by the federal government, according to a Productivity Commission report, that found:
- 65 per cent of people seeking emergency hospital treatment received it on time last year (down 17 percentage points in nearly a decade)
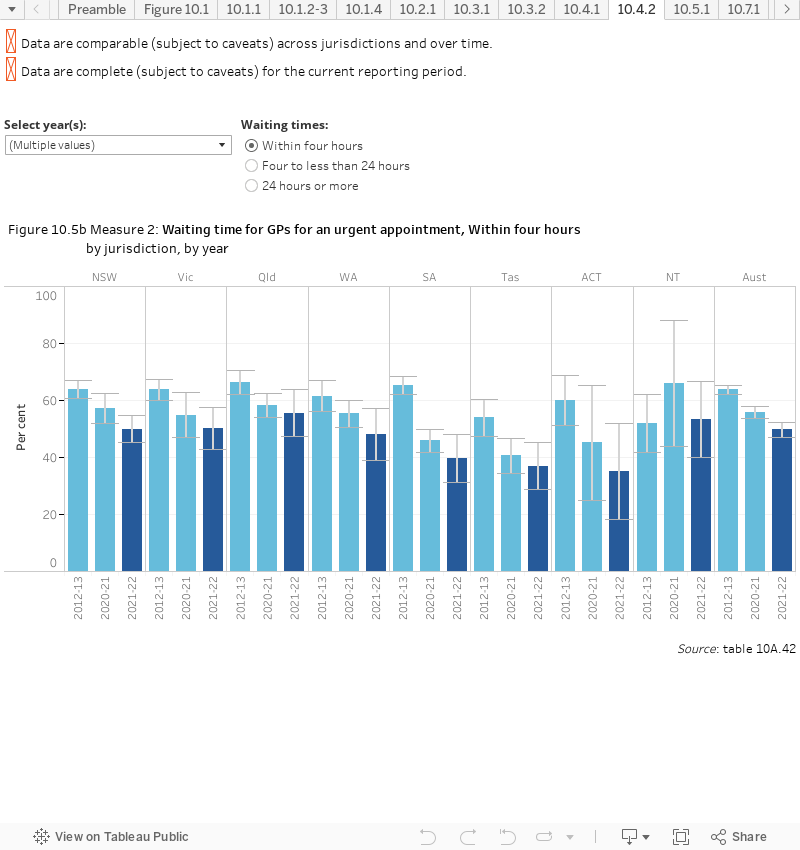
- 39.1 per cent of patients seeking emergency treatment from a GP had to wait one day or more (up 5.2 per cent)
- 5.6 per cent of Australians delayed filling a prescription last year because of cost concerns, the first increase recorded in 10 years of data.
The blowouts are despite spending on hospitals and primary care (which includes GPs) rising by more than $9 billion, with long-term indications the system will become more stressed as fewer doctors enter general practice.
A new blame game
State premiers are laying the blame on the federal government and want more funding for hospitals (which rose briefly from 45 to 50 per cent when COVID-19 struck) and GPs, a shortage of which they say is overloading emergency rooms.
“It’s not our job,” Victorian Premier Daniel Andrews said this week. “We’re essentially doing some of the federal government’s work for them.”
The former head of the federal government’s Department of Health, Stephen Duckett, told The New Daily that some “public posturing” was to be expected before meetings like Friday’s national cabinet.
“They’re going into the meeting saying, ‘Give us a whole lot more money’,” Dr Duckett said.
“I like to go into meetings and ask for a whole lot more money, too, but if I were […] the Prime Minister, I would essentially say, ‘Well, what are you doing in return?’
“Over my lifetime, generally, if you pour money into hospitals to reduce waiting lists, they actually don’t.”
The federal government is rolling out urgent care clinics that will stay open late and see people with non-life threatening conditions, such as broken bones, that would usually be treated in emergency rooms.
“Our government is not simply going to be adding more money to the existing structures,” Health Minister Mark Butler said last month.
Victoria and New South Wales have been enthusiastic adopters of the idea and established 50 of their own to match the federal government’s contribution, but only budgeted to run them for 18 months in what some observers see as a ploy for future funding.
Mr Butler is holding back something too: Last week he announced plans for a shakeup of Medicare funding he dubbed the most far-reaching in its near 40-year history.
But he hasn’t yet released the blueprint of his Strengthening Medicare taskforce, which has a budget of about $250 million a year.
Mr Albanese has said that it will be presented to the state premiers on Friday.
|
Major revamp on the way for Medicare
10 News First – Disclaimer |

|
New model needed
Jane Hall, a distinguished professor of health economics at the University of Technology Sydney, says Rudd government reforms of hospital funding had brought an end to a familiar ritual of state and federal governments bickering about money.
“COVID has upset all that,” Professor Hall said.
People are seeking treatments that had been delayed or deferred, and more money is being sunk into measures such as infection control.
“We’ve got governments who’ve had to bail out all sorts of activities so expenditure across a whole range of areas has gone up, and (states and the Commonwealth) are feeling the pinch.”
But she says most of all the pandemic has put a fine point on big trends that were emerging long before its onset: Australians are living longer and with the benefit of expensive improvements in drugs and technology.
That means, she says, they need treatments that range across the three divisions of government funding on which Medicare is built: Prescriptions, hospital and primary care.
“Suppose you want to lose weight. [The GP] can’t say, ‘look, I’ve got an exercise physiotherapist in the practice’ … [or say that] ‘instead of prescribing a drug for you it would be more cost-effective for society [for] you to have regular physiotherapy sessions’. That can’t happen currently, but it also can’t change in one fell swoop,” she said.
“We’ve got a health system that was designed very well for the late 20th century, but things have moved on.”







